Everyone knows cigarette smoking is dangerous and even deadly. We hear about the dangers from our doctors, teachers and parents, and we see warning labels on the packages “May cause cancer”. So why do people even smoke cigarettes? Why do approximately 3,000 teenagers begin smoking or using tobacco products each day? And why do over 45 million American adults still smoke, even though they may try quitting many times? There must be a reason why 31 million American adults want to quit smoking, but only about 5% are successful after one year.
The answer lies with a single molecule: nicotine. This natural ingredient is found in all tobacco products and can cause intense addiction. With repeated use, tobacco products can also lead to a host of deadly diseases such as cancers of the lung, mouth, and pancreas, Emphysema, heart disease, and Stroke. As the noted tobacco researcher M. A. H. Russell once wrote,
“There is little doubt that if it were not for the nicotine in tobacco smoke, people would be little more inclined to smoke than they are to blow bubbles or to light sparklers.”
So what is nicotine and how does it lead to addiction? In this module, the following questions are answered:
- What is nicotine?
- How does nicotine enter the body?
- How does nicotine affect the brain?
- Why does nicotine make some people feel good?
- How does repeated use of nicotine products change the brain?
- What are the stages leading to nicotine addiction?
- Are teens more likely to become addicted than adults?
What is nicotine?
One of the most abundant and highly addictive chemicals found in tobacco products is nicotine. Nicotine is found in high quantities in the tobacco leaves. Each tobacco product contains different amounts of nicotine, but on average, a typical cigarette contains about 10-15 mg, with the average smoker inhaling approximately 1-2 mg of nicotine.
At high doses, nicotine can be extremely poisonous. In fact, nicotine was previously used in insecticides to destroy insects, but its use as an insecticide was banned in the US in 2001 due to contamination of food products. Ingestion of high doses of nicotine causes vomiting, tremors, convulsions, and even death in a short amount of time.
To put this in perspective, just one drop of pure nicotine can kill a person and 60 mg can be deadly. A small child or animal can become very sick or even die from eating just one cigarette left unattended. While ingestion of high doses of nicotine is not very common, the repeated use of products that deliver small amounts of nicotine can lead to a disease called addiction.
How does nicotine enter the body?
Depending on the tobacco product used, nicotine can enter the body various ways. Cigarette smokers inhale nicotine from the smoke into their lungs. Smokeless tobacco users absorb nicotine through the skin and mucous membranes of the mouth. Nicotine can also enter through the mucous membranes in the nasal cavity (nose) if the oral form of dry snuff is used. Lastly, nicotine can be absorbed through the skin with use of products such as the nicotine patch. Regardless of the means of entry, nicotine quickly enters the bloodstream, where it can then be distributed throughout the body. As smoking is the most common route of entry for nicotine, it will be discussed it in more detail below.
“Very few customers are aware of the effects of nicotine, i.e., its addictive nature and that nicotine is a poison.“
(1979 tobacco company Brown and Williamson document)
The amount of nicotine a person inhales from a cigarette depends on the smoker’s puffing behavior. A person who takes deep and frequent puffs on a cigarette will inhale more nicotine than a person taking short little puffs. On average, a smoker will take about 10 puffs per cigarette to deliver 1-2 mg of nicotine.
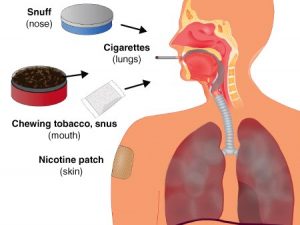
Figure 1.1 Four main routes of entry for nicotine. Regardless of the route of entry, nicotine gets into the bloodstream.
Once inhaled, the nicotine travels immediately to the lungs where it reaches millions of tiny air sacs called alveoli. There are over 480 million tiny air sacs or alveoli that participate in the air exchange process in the lungs. If all the alveoli were laid side by side they would cover an area the size of a tennis court!
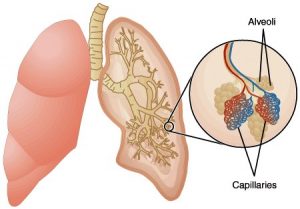
Figure 1.2 The structure of the lungs. Air exchange occurs at the site of the alveoli (tiny air sacs) that are covered with small blood vessels (capillaries).
Each air sac is covered with tiny (blood vessels) through which the blood flows. The large number of alveoli provides ample space (surface area) for oxygen and carbon dioxide exchange. At the site of the alveoli, oxygen, which is breathed in from the air, is absorbed into the bloodstream. At the same time, is generated by all cells, travels in the bloodstream to the lungs, where it is exhaled. Likewise, the large surface area of alveoli allows for efficient delivery of nicotine into the bloodstream. Once nicotine enters the bloodstream, it then travels very quickly throughout the body and affects many regions.Each air sac is covered with tiny (blood vessels) through which the blood flows. The large number of alveoli provides ample space (surface area) for oxygen and carbon dioxide exchange. At the site of the alveoli, oxygen, which is breathed in from the air, is absorbed into the bloodstream. At the same time, is generated by all cells, travels in the bloodstream to the lungs, where it is exhaled. Likewise, the large surface area of alveoli allows for efficient delivery of nicotine into the bloodstream. Once nicotine enters the bloodstream, it then travels very quickly throughout the body and affects many regions.
Each air sac is covered with tiny Capillaries (blood vessels) through which the blood flows. The large number of alveoli provides ample space (surface area) for oxygen and carbon dioxide exchange. At the site of the alveoli, oxygen, which is breathed in from the air, is absorbed into the bloodstream. At the same time, Carbon dioxide is generated by all cells, travels in the bloodstream to the lungs, where it is exhaled. Likewise, the large surface area of alveoli allows for efficient delivery of nicotine into the bloodstream. Once nicotine enters the bloodstream, it then travels very quickly throughout the body and affects many regions.
Figure 1.3 Nicotine absorption into the bloodstream from the lungs. The huge surface area of the alveoli is a very efficient way to get nicotine into the bloodstream.
How does nicotine affect the brain?
One of the first areas to which nicotine travels is the Brain. Regardless how nicotine enters the body (inhalation, mouth, nose, or skin), it will be absorbed into the bloodstream and reach the brain quickly. The fastest way to get nicotine to the brain is to inhale it—it only takes about 10 seconds for nicotine to reach the brain. This is because the blood from the Lungs travels to the Heart, which then pumps the blood through the Arteries to all major organs, including the brain. 
Figure 1.4 Path that nicotine travels from the mouth to the brain. Nicotine is inhaled from cigarette smoke and travels directly to the lungs, where it is immediately absorbed into the bloodstream. Once in the blood, nicotine travels to the heart, where it is then pumped throughout the entire body, including the brain.
The brain is the master control center
Once nicotine reaches the brain, it triggers a series of responses that alters the way cells in the brain communicate with each other. A brief review the function of the brain will help in understanding how nicotine causes its effects.
The brain is an amazing part of the body—it’s composed of billions of tiny cells called Neurons, which communicate with each other to control all functions throughout the body. The brain regulates all aspects of life – pumping of the heart, breathing, walking, emotions, and memories. The brain is what differentiates humans from all other types of living species—humans are the only species to rationalize situations, have wild imaginations, and perform high level thoughts and tasks.
How do neurons communicate with each other?
One of the primary effects of nicotine is to alter the way that neurons (i.e., brain cells) communicate. Neurons communicate with each other through both electrical and chemical signals. Each neuron consists of a Cell body (the main part of the neuron that contains the nucleus, or the cell’s control center), an Axon, and many Dendrites. The axon is one long extension from the cell body that carries electrical signals from one end of the neuron to the other end (referred to as the terminal). These signals travel extremely fast–up to hundreds of miles per second. Dendrites are shorter extensions that also branch off the cell body. Think of the dendrites as tree roots that branch out. The dendrites receive signals from other neurons in the form of chemicals.

Figure 1.5 Neuron structure. Each neuron consists of a cell body attached to one long axon and several shorter dendrites.
Neurons communicate information to each other when they are in close contact. The connections between neurons are called synapses. On average, one neuron can form about 1,000 Synapses with other neurons. With millions of neurons forming thousands of neural connections, it is estimated that the number of neuron-to-neuron connections in the brain exceeds the number of stars in our galaxy.

Figure 1.6 The synapse—the connection between two neurons. The synapse is the location where communication between neurons occurs. The arrow shows the direction in which information (i.e., electrical activity) flows.
So how does the communication work at the synapse? First, an electrical impulse travels down the axon toward the terminal. Once there, the electrical signal triggers the release of chemicals called Neurotransmitters from tiny sacs into the synaptic space outside the terminal. These chemicals actually carry the “messages” from one neuron to another. Once in the synaptic space, the neurotransmitter attaches to specific proteins called Receptors on the dendrites of the neighboring neuron. There are thousands of receptors on the dendrites, with each type of receptor recognizing only a very specific neurotransmitter, similar to a lock and key. When the neurotransmitter binds (or attaches) to a specific receptor, the receptor will either increase or decrease the electrical activity of the neuron on which it resides.

Figure 1.7 Neurons communicate at the synapse. Neurotransmitters are released from vesicles in the terminal to the outside of the neuron. The neurotransmitters then bind to receptors on a neighboring neuron’s dendrites, causing a cellular response (a change in electrical activity).
Let’s consider one of the major neurotransmitters in the brain called Acetylcholine. Interestingly, nicotine mimics this neurotransmitter. Nicotine acts just like acetylcholine, but works even better. This is described below. Acetylcholine binds to receptors (“acetylcholine receptors”) that increase the electrical activity of neurons, resulting in more signals transmitted to neighboring neurons. Once acetylcholine has done its job, it is destroyed. New acetylcholine must be made by the cells to repeat the whole process.
Nicotine increases electrical activity in neurons to cause several effects
As previously mentioned, nicotine mimics the effect of the neurotransmitter acetylcholine. When nicotine enters the brain, it can actually bind to the same receptors that bind acetylcholine. For this reason, the acetylcholine receptor is often referred to as a Nicotinic receptor.
However, when one uses a tobacco product or another nicotine containing product, there is more nicotine available in the synaptic spaces compared to acetylcholine. The nicotine competes with acetylcholine to bind to the nicotinic receptors and it wins. Now, with more nicotinic receptors activated by nicotine, a more intense response is produced.
So while acetylcholine normally provides the just the right amount of alertness when it b
inds to its receptors, nicotine produces a much more intense response (increased alertness, pleasurable feelings) due to its higher concentrations at the acetylcholine receptors.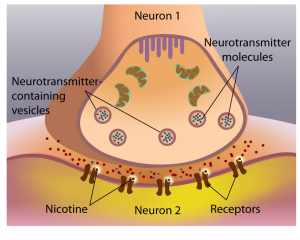
Figure 1.8 Nicotine competes with acetylcholine to increase electrical activity in neurons. Since there is more nicotine in the synaptic space, it wins, and produces larger electrical currents, and heightened responses.
Review the entire process of how neurons communicate and the effect of nicotine.
Nicotinic receptors are found in many other regions of the body besides the brain. Not surprisingly, nicotine acts in the body wherever nicotinic receptors are found, such as on the heart, blood vessels, and muscles. The widespread distribution of nicotinic receptors explains why nicotine will increase heart rate, blood pressure, and muscle contractions.
Why does nicotine make some people feel good?
When some people use a product containing nicotine, they feel good. Others do not—so they do not continue to use the product. But for those individuals who do like the effect of nicotine, they will continue to smoke or use nicotine-containing products. So what causes the feeling of pleasure in some tobacco users?
There is a group of neurons that forms a pathway located in the middle of the brain called the “reward pathway” or the “pleasure pathway.” The reward pathway is activated by natural rewards like food and water. Activation of the pathway by natural rewards gives us the feeling of wanting more, a necessary function to ensure our survival as a species. But drugs are even better activators of the pathway.
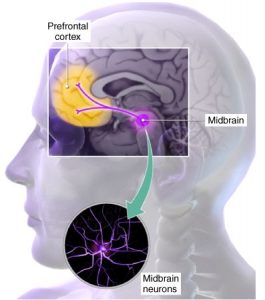
Figure 1.9 The reward pathway. The reward pathway begins in the midbrain where cell bodies of neurons send long fibers to the prefrontal cortex. Think of the midbrain cell bodies like airline hubs whose airline routes (neuron fibers) extend to the coastline (pre-frontal cortex). Nicotine and other addictive drugs act on receptors in this pathway that activate rewarding feelings.
For example, nicotine activates the pathway by triggering the release of another neurotransmitter called Dopamine. Dopamine has been termed the “pleasure neurotransmitter” because it causes pleasurable feelings when it binds to its receptors (“dopamine receptors”) in the reward pathway.
Once activated by nicotine, the reward pathway transmits information that we perceive as feelings of pleasure, and just feeling really good. Nicotine acts in other parts of the brain to reduce anxiety and stress.
Scientists have discovered that this same reward pathway is also activated by drugs like alcohol, cocaine, and heroin. This discovery explains why nicotine and other drugs that produce rewarding feelings can be a first step toward addiction.
However, nicotine effects are short lived because the drug is quickly metabolized (broken down) in the body. Thus, when nicotine is no longer present, the pleasurable experience decreases and nicotine users feel the need for more nicotine in the body just to function normally, so they smoke another cigarette.
How does repeated use of nicotine change the brain?
When one continues to use a product with nicotine in it, a strange thing happens. The number of nicotinic receptors—that is, acetylcholine receptors—increases on the neurons! With more receptors present, the person needs more acetylcholine binding to them to feel normal. But the neurons can only make so much acetylcholine. So what is the result? The person needs more nicotine to feel normal.
When the nicotine is not present, a person will often get symptoms such as headaches, tremors, shakiness, and an overall feeling of irritability and frustration. To get rid of these “Withdrawal” symptoms, the user will smoke another cigarette or use another tobacco product and begin to feel much better. The presence of withdrawal symptoms is typical of dependence and it almost always precedes Addiction.
In addition, the increased nicotinic receptors can also explain Tolerance, or the need to use more of the product containing nicotine to get the original effect. The distinction among tolerance, dependence, and addiction is explained in detail below.

Figure 1.10 Nicotine causes changes in the brain. A section of the front of the brain is shown from a non-smoker and a smoker. The number of nicotinic receptors (in yellow and red) is significantly increased in the smoker compared to the non-smoker. (From Perry et al., 1999)
The good news is that the increase in receptor number is probably not permanent. Once one stops using a product containing nicotine, the number of receptors will return to normal pre-nicotine levels—although this could take more than a year. However, immediately after stopping smoking for example, many users experience unpleasant withdrawal symptoms because the brain now has an excess of nicotinic receptors, which are unoccupied. The long process for the brain to recover to normal is one reason why many people who try to quit using nicotine products can’t get past the first year (or even week!) nicotine-free.
What are the stages leading to nicotine addiction?
When a person uses a drug with rewarding properties (like nicotine, alcohol, or cocaine), they are at risk for addiction. Although they don’t become addicted immediately, there are 2 stages that usually precede addiction—these include tolerance and dependence. Let’s review the sequence in the context of smoking cigarettes (although it’s the same for any tobacco product).
Stage 1: Tolerance
After smoking only a few cigarettes, nicotine loses its effectiveness at stimulating the reward pathway. Scientists have shown that the nicotinic receptors can lose their sensitivity to nicotine. Now, the person must smoke more cigarettes because more nicotine is necessary to cause the same effect. This smoker has become tolerant to nicotine, which usually happens first, even before dependence sets in.
Stage 2: Dependence
As the smoker continues to smoke, the smoker becomes dependent on nicotine. Dependence means that the smoker requires nicotine just to function normally. So, if a dependent smoker were to stop smoking, he/she will experience withdrawal. The symptoms of nicotine withdrawal can range from mild to severe and include anxiousness, inability to sleep, and depressed mood. Withdrawal can begin within as little as a few hours after the last cigarette. Without thinking about it, people smoke enough cigarettes or use enough tobacco products (i.e., chewing tobacco, etc.) each day to keep the levels of nicotine in their brain at a relatively constant level and to feel the effects all day long.
Stage 3: Addiction
Once the smoker shows nicotine tolerance and dependence, addiction follows. Addiction to nicotine occurs when a person becomes a Compulsive tobacco user and can no longer control how often he/she uses tobacco—regardless of the negative consequences. Addiction can creep up quickly (some recent evidence suggests addiction could begin as soon as 2–3 weeks from use of the first cigarette), or it could occur over a longer period. The user is not really aware it is happening, but there are some symptoms.
The most obvious symptoms include:
- the person can’t control when he/she smokes a cigarette or uses tobacco products (compulsive use)
- constant thoughts about getting a cigarette or other type of tobacco product
- craving that results when he/she can’t get nicotine that’s contained in the product
“The desire to quit seems to come earlier now than before, even prior to the end of high school… attempts to quit are very painful, they thought they could quit easily, but they soon learn…” they have become SLAVES to their cigarettes.
(Imperial Tobacco)
Often people who are addicted to nicotine think that they can control their smoking, and can quit any time. However, if they quit, withdrawal symptoms emerge first and then craving results. Craving (and stress!) almost always leads the person to relapse, and he/she starts smoking again. The person who starts smoking by age 19 typically takes about 20 years to finally quit.
Sequence of stages leading to addiction
- Tolerance occurs when smokers require more nicotine just to have the same effect they felt initially. It usually precedes dependence.
- Dependence occurs when smokers require nicotine just to function normally
- Tolerance and dependence lead to nicotine addiction—one can’t quit.
Are teens more likely to become addicted than adults?
For years, people have noticed a remarkable difference between a child’s or a teenager’s decision-making ability and that of an adult. However, only recently scientists discovered a biological explanation for this difference. The brain continues to develop and mature until about the mid-20’s, with the most dramatic changes occurring during adolescence. The major changes happen during the teen years in the part of the brain called prefrontal cortex, which is responsible for functions such as self-control, judgment, thinking, emotions, and decision making.
Because the prefrontal cortex is still maturing, teenagers are more likely to make poor decisions such as trying drugs or alcohol without fully comprehending the long-term consequences. You might remember that the Prefrontal Cortex is the place in the brain that the reward pathway terminates (see Figure 1.9).

The human brain is not fully mature until the mid-20’s, thus leaving teenagers more vulnerable to developing a nicotine addiction.
The teenage brain is extremely vulnerable to nicotine and other addicting drugs
The teenage brain is particularly vulnerable to drugs such as nicotine and alcohol. These drugs can have much more dramatic consequences on the developing brain than in an adult brain. How do we know this?
Here’s what we know about smoking and human brains: Both adults and teen smokers show increased nicotinic receptors in their brains compared to non-smokers. Scientists use a type of brain scan called a PET scan to look for receptors in the brain. A typical PET scan of nicotinic receptors in human brains shows the difference between smokers and non-smokers (adults or teens).
Even more information about adolescent brains can be learned from animals. Many animals have a similar brain structure to humans and serve as an excellent model to study human diseases. For example, scientists gave nicotine (by injections) to adolescent rats and found the same increased number of nicotinic receptors in rat brains as seen in human brains. But, they were able to show something even more interesting.The increase in nicotinic receptors in the adolescent rat brain occurred more rapidly compared to the adult rat brain, and the young brains did not recover to normal as easily.
So the animal studies provide a clue as to what occurs in humans. It is difficult to do these kinds of studies in adolescent humans, so we must rely on data from the rats. Nevertheless, it is clear that the adolescent brain structure changed after exposure to nicotine. The nicotine-induced increase in the amount of nicotinic receptors at this early age suggests that adolescents can become addicted to nicotine fairly easily.

Reasons why teens become addicted to nicotine more easily than adults:
- The region of brain that controls judgment and decision-making is not completely developed in teens
- The increase in the number of nicotinic receptors in adolescent brains occurs more rapidly, and persists, compared to adults. More receptors lead to the need for more nicotine.
Teen smoking and addiction statistics
The following lists national trends for smoking behavior in teenagers (reported as of 2007).
Reasons why teens become addicted to nicotine more easily than adults:
- 90% smoking adults begin smoking by age 21, one half of adult smokers are addicted before their 18th birthday.
- Every day, 3,200 children between ages 12-17 smoke their first cigarette.
- 1,300 of those smokers will become addicted.
- Half of those will die from smoking.
- If smoking trends remain the same, over 6.4 million current teen smokers will die prematurely from smoking related causes.
- Smoking rates are declining in teenagers.
- Teen smoking is associated with many other unhealthy activities, such as carrying weapons, trying different drugs, fighting and engaging in high-risk sexual activity.
- Smoking teens are three times more likely to drink alcohol, eight times more likely to smoke marijuana, and 22 times more likely to try cocaine.
- Teens are more likely to develop a severe addiction to tobacco than if they begin smoking later in life.
- 50% of smoking teenagers have unsuccessfully tried to quit, failing to break the addiction.
- 5.6 million children alive today will ultimately die from smoking
Now that you’ve read through the content section, you can check your answers to Mission 1 here