P.A.D. (aka ‘sedation’)
Pain, agitation, and delirium management in the ICU
Christopher Cox, Bridgette Kram, Nick Wysham
Goal: Expedite recovery and decrease likelihood of setbacks.
That is, the overarching goal is to provide life support only for as long as needed, keeping a patient’s mental function as clear as possible throughout while also encouraging participation in mobility protocols. Read: limit sedatives, maximize mobility, and limit exposure to invasive life support, catheters, and potentially toxic drugs.
Ancient history / background
Not long ago, common practice was to deeply sedate patients with continuous benzodiazepine and opioid drips. The belief was that being on a ventilator was so traumatic that people needed to be nearly comatose so that they wouldn’t suffer.
Over time however, a number of trends have emerged that challenged that belief system based on the findings of some landmark studies listed at the bottom of the page. One was that a daily cessation of sedatives and analgesics with the goal of allowing a ‘daily awakening trial,’ aka ‘spontaneous awakening trial (SAT),’ was quite effective in reducing the duration of ventilation. While being on a ventilator can certainly be traumatic, subsequent research showed that lighter levels of sedation did not increase the risk of post-discharge PTSD, depression, or anxiety symptoms. In fact, sedative-driven, delirious, non-factual memories increase the risk of PTSD in comparison to factual ICU memories–even if they are somewhat unpleasant factual memories.
And when combined with a spontaneous breathing trial (SBT; a test of readiness for extubation), things went even better…almost as if 1 + 1 = 3 in terms of ventilator days averted.
Subsequent findings confirmed that delirium was extremely common in the ICU, was promoted by sedatives such as benzodiazepines, and was an independent risk factor for death. By extension, patients cannot participate effectively in their own ventilation if they are sedated. They also cannot participate in physical therapy.
Yet said in a different way, the longer a person is in the ICU on a ventilator, the greater is their risk for: death, complications from invasive monitoring and tubes (i.e., CLABSIs, UTIs, VAPs, pressure ulcers, etc), delirium, long-term physical disability, long-term psychological disability, and on and on. This is where protocols came in.
Why do we need a protocol for pain, agitation, and delirium (PAD)?
In the absence of a PAD protocol, we often make 2 serious mistakes that can lead to poor outcomes:
- We use too little drug up front for acute needs, often just uptitrating a drip.
- As a result of #1, we soon find ourselves on high doses of continuous drugs with no good plan for how to reduce / remove them as the patient improves.
Protocols help us to avoid #1 and #2.
Think of the PAD protocol as a safety net, a collection of best practices, and a way to introduce protective redundancy in a complex system with multiple moving (human + computer) parts. It also allows all providers to speak a common language. The quality of care you deliver is only as good as the weakest link! We think that if we become truly expert in this protocol, which should work for >90% of patients, then we are offering the best to our patients. We don’t forget how to manage special cases, but reserve the ‘off the grid’ stuff for unique issues. Conceptually, we can either choose to focus our efforts on the 90%, or we become trapped by always considering every odd case and exception (the trap of academia gone awry).
But I’m a trainee–why can’t I just manage sedation by myself?
We think that learning a protocol will allow you to become well versed in the state of the art management of critically ill patients. There is flexibility within the protocol as well. There are many opportunities to individualize the protocol more tightly to the situation you observe at the bedside. Provider variability in care is the source of much confusion among ICU team members. If everyone did things differently, how could we possible to the right thing consistently?
Also, this can be hard! Even though we have a protocol, many patients don’t completely follow the rules…as you will find out in rounds. We are all constantly learning how to do this challenging part of critical care better. It takes a team!
How do we measure our progress in PAD—what is the PAD language?
This is a pain, agitation, and delirium (PAD) protocol that is designed to target specific pain (Numeric Rating Scale (NRS) or Critical care Pain Observation Tool (CPOT)) and agitation (Richmond Agitation and Sedation Scale (RASS)) goals set by the physician. We assess for the presence of delirium using the Confusion Assessment Method-ICU (CAM-ICU) scale. Note that the acronym is PAD…not APD or DAP. We must stress that P>A>D is the order that we administer medications as you will now see:
Pain: Our gold standard for pain measurement is patient self-report. If patients are lightly sedated, they can often report their pain on the NRS (range 0 – 10). Therefore, we should encourage this. For ventilated patients who are unable to self-report we use the CPOT, which ranges from 0 (unlikely to have pain) to 8 (very likely to be in pain). Our typical goal is a CPOT <3.


Agitation: We manage agitation using sedatives once the patient’s numerical pain scale or CPOT is within target range (CPOT <3). We assess the level of sedation using the RASS. In general, we target a RASS of 0 to -1. Note that you can order the RASS target to be lower if needed (e.g., severe hypoxemia). This graphic is from Dr. Wes Ely (ICUdelirium.org).
Delirium: Once the RASS target is attained, we also assess for the presence of delirium using the CAM-ICU scale. If patient is ‘CAM positive,’ we think through non-pharmacologic and pharmacologic interventions to address the presence of delirium. This graphic is from Dr. Wes Ely (ICUdelirium.org).
How does the PAD protocol work?
Here are links to PDF versions of the PAD protocol for (a) opioid-naive patients and for (b) opioid-tolerant patients.
But here is a simplified overview in 3 steps.
- Pain:
– review home meds to make sure a patient’s usual opioid dose is being considered. Don’t be stingy to a chronic opioid user!
– Don’t forget a bowel regimen! Start early.
– Load with fentanyl (preferred) IV boluses q15 minutes PRN or hydromorphone IV boluses q30 minutes PRN to reach CPOT <3
– If 3 or fewer doses are sufficient (i.e., pain is well controlled), move to maintenance PRN pathway
– if boluses aren’t sufficient, transition to fentanyl drip
– Increase drip if more prn boluses are required
– Decrease drip if at CPOT and RASS at goal for 4 hours; if on sedative, decrease sedative drip first
- Agitation
– Specify RASS target in Epic order (usually 0 to -1)
– if CPOT<3 but RASS is above goal, add propofol
– you can use dexmedetomidine if anticipated short course, failure of other strategies, or contraindication to propofol
– lorazepam can be used as a prn if propofol and dexmedetomidine are insufficient / contraindicated (lorazepam is 4th line, if you will)
– think through possible relative contraindications (e.g., hypertriglyceridemia with propofol; bradycardia with dexmedetomidine)
– decrease sedative if stable (propofol can be titrated q5 minutes; dexmedetomidine can be titrated q15 minutes)
- Delirium
– First, think through non-pharmacological approaches to delirium management (quiet times, open blinds during day, reduce noise at night, provide glasses/hearing aids, etc).
– Early mobility is a great way to address delirium!
– Second, consider the use of antipsychotics (assuming QTc is normal). Please work with the MICU pharmacist and attending on this.
– Click here for a great video on ICU delirium
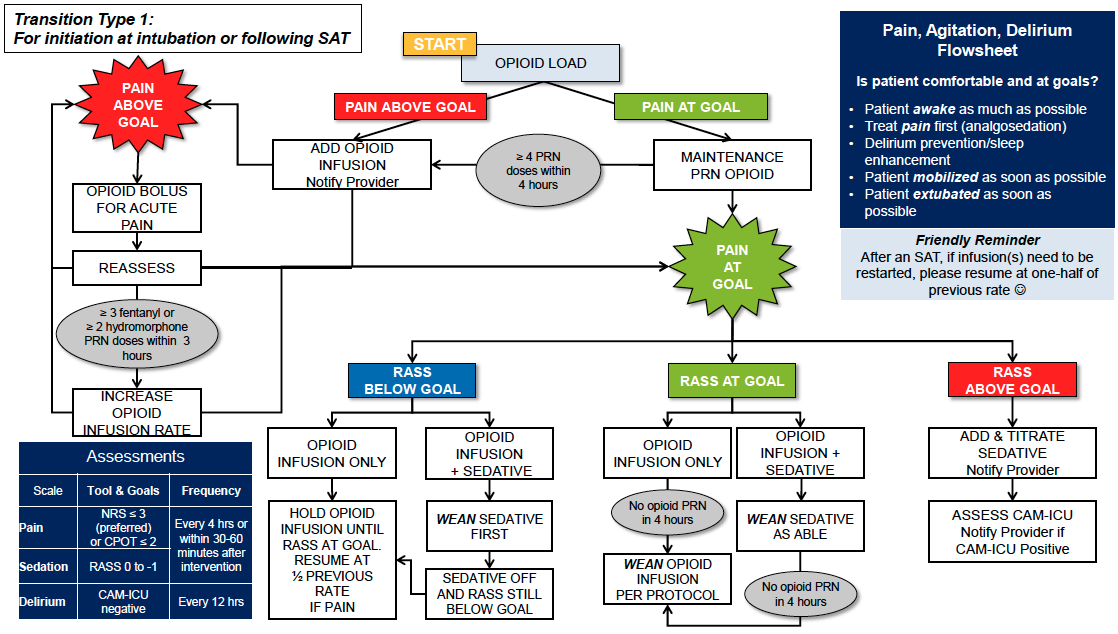
More details: initiating PAD at intubation or after SAT (Type 1) vs. initiating PAD while already on drips (Type 2)
These graphics show a flow chart the slightly different way PAD is handled based on the situation at which it is initiated. They can be viewed in higher resolution by clicking here.

{kind=link}
{kind=link}

Who should be on the PAD protocol?
By default, we think that the PAD protocol should be ordered on every ventilated patient with these exceptions:
– HFOV
– status epilepticus
– severe alcohol withdrawal
– neuromuscular blockade
– targeted temperature management
– refractory intracranial hypertension
How do I manage challenges?
First rule: try not to discontinue PAD if possible. If you need deeper sedation, for example in severe ARDS, then simply adjust the target RASS goal. Please do this before just discontinuing the protocol. Because later on when the patient improves, you may notice that they have had no ‘backoff plan’ for drips for a few days likely—and now are deeply sedated (soon to be followed by very delirious).
Communication is also key. Work with the nursing staff to understand their perceptions. Be a team! Be sure everyone knows what the targets are. Also understand how many (or few) prns are being given.
Look for opportunities to simplify wherever you can (stop drips, d/c lines, etc)!
How can I learn more:
Here is a link to a critical care grand rounds introduction of PAD.
Here is a link to a nice power point overview of PAD, its justification, and other Duke-centric stuff.
How does the PAD protocol work best?
We first have to order the protocol in Epic!
We discuss the NRS / CPOT and RASS targets with the attending, fellow, and bedside nurse.
We review the NRS/CPOT, RASS, and CAM-ICU scores/status on rounds every day. MDs, RNs, RTs, pharmacists, and others may have suggestions for targets based on their perspectives. If our goals change, we must change the order in Epic immediately (e.g., changing RASS target).
How do I order the PAD protocol in Epic?
We thought you’d never ask. Written versions of the protocols can be seen for opioid-naive and opioid-tolerant patients by clicking the links. But here is an Epic walk through…











Recent high impact research on pain, agitation, and delirium
In this large, propensity-matched ICU population, patients treated with propofol had a reduced risk of mortality and had both an increased likelihood of earlier ICU discharge and earlier discontinuation of mechanical ventilation.
A very important paper that linked delirium to mortality.
Very interesting counterpoint trial to the complete daily interruption strategy of sedation. In this Canadian Clinical Trials group RCT, for mechanically ventilated adults managed with protocolized sedation, the addition of daily sedation interruption did not reduce the duration of mechanical ventilation or ICU stay.
Here are links to 2 neat papers that take on Ten Myths Regarding Pain in the ICU and Ten Myths Regarding Sedation in the ICU.